 Facebook
Facebook  Twitter
Twitter  Soundcloud
Soundcloud  Youtube
Youtube  Rss
Rss 
As of early December 2021, nearly 70.4% of Indonesians had received one dose of an approved COVID-19 vaccine. Particularly considering the arrival of the Omicron variant in Indonesia, this is certainly cause for celebration. But this figure obscures important sources of discrepancies: while nearly all eligible adults in Jakarta are reported to have received at least one dose, less than a quarter of those in Papua have done so, for instance.
Geography is only one axis of inequality, however: other sources of vaccination inequity are less easy to measure. Part of the problem may stem from inequality in access, as some people may simply continue to have a better chance to get the jab than others, owing to connections or willingness to pay. Over the last year, governments across the world were embroiled in scandal as they offered differential access to vaccines to wealthy individuals. Looking at Indonesia, in particular, Lila Sari has documented how political parties in Indonesia have played a crucial role in vaccine delivery—doling out jabs to supporters as a means of shoring up votes.

Misinformation & government inaction fuel vaccine hesitancy in the Philippines
95% of hundreds of thousands of internally displaced people in resettlement sites built after Typhoon Haiyan in 2013 are not vaccinated.
But inequities may also arise from certain groups being more susceptible to forms of misinformation that discourage people from getting vaccinated. As Najmah, Sharyn Davies, and Kusnan describe in the New Mandala last May, members of Indonesia’s marginalized populations are some of the most vulnerable to misinformation surrounding vaccines—such as the concern that the Chinese vaccine Sinovac may contain pork products and thus be forbidden (haram).
Data availability is a major difficulty in adjudicating the extent of these problems: while publicly reported data indicates the overall uptake of vaccines according to region and occupation, we know very little about the sorts of individuals receiving these jabs. More concerningly, we know even less about those individuals who do not wish to receive a vaccination. Identifying and reaching these uninoculated populations is particularly crucial as the pandemic continues to drag on, and vaccination remains the best tool for combatting serious illness.
To fill in these gaps, we analyzed data from two nationally representative surveys of Indonesian adults conducted in March (N = 1,064) and October 2021 (N = 981). These data offer a unique window into how Indonesia’s vaccination campaign is being received by the individuals it intends to reach. We seek to answer several related questions. Firstly, which groups are getting vaccinated? Secondly, which groups are expressing an interest in getting the vaccine, but not able to do so? And finally, why is it that some people do not want the vaccine? We take up these questions and consider the implications for the equitable roll-out of vaccines in Indonesia.
We home in on one particularly concerning finding: as of October 2021, older Indonesians, the most vulnerable segment of society, are the least likely to be vaccinated and the least interested in seeking out the jab. The role of misinformation looms large in this finding, as it appears the tendency for older Indonesians to resist inoculation is a function of their lower levels of education than younger cohorts. Developing strategies to reach this population is particularly crucial for stemming the tide of the pandemic.
Who is getting vaccinated in Indonesia?
Our survey finds that in early October 2021, 42.1% of adult Indonesian had received at least one dose of a vaccination—slightly higher than officially reported statistics. In Figure 1, we show the percentage point increases for individuals in different subgroups—according to income, education level, age, and geography. In March 2021, no subgroup reported more than 5% vaccination rates. As the roll-out of vaccines took place of the past 6 months, however, stark differences in vaccination rates have emerged: richer and better educated Indonesians have outstripped their poorer and less educated counterparts in the rush to obtain vaccinations. By October 2021, for instance, 71.2% of college graduates had received at least one jab, compared to 15.4% of those with no formal education.
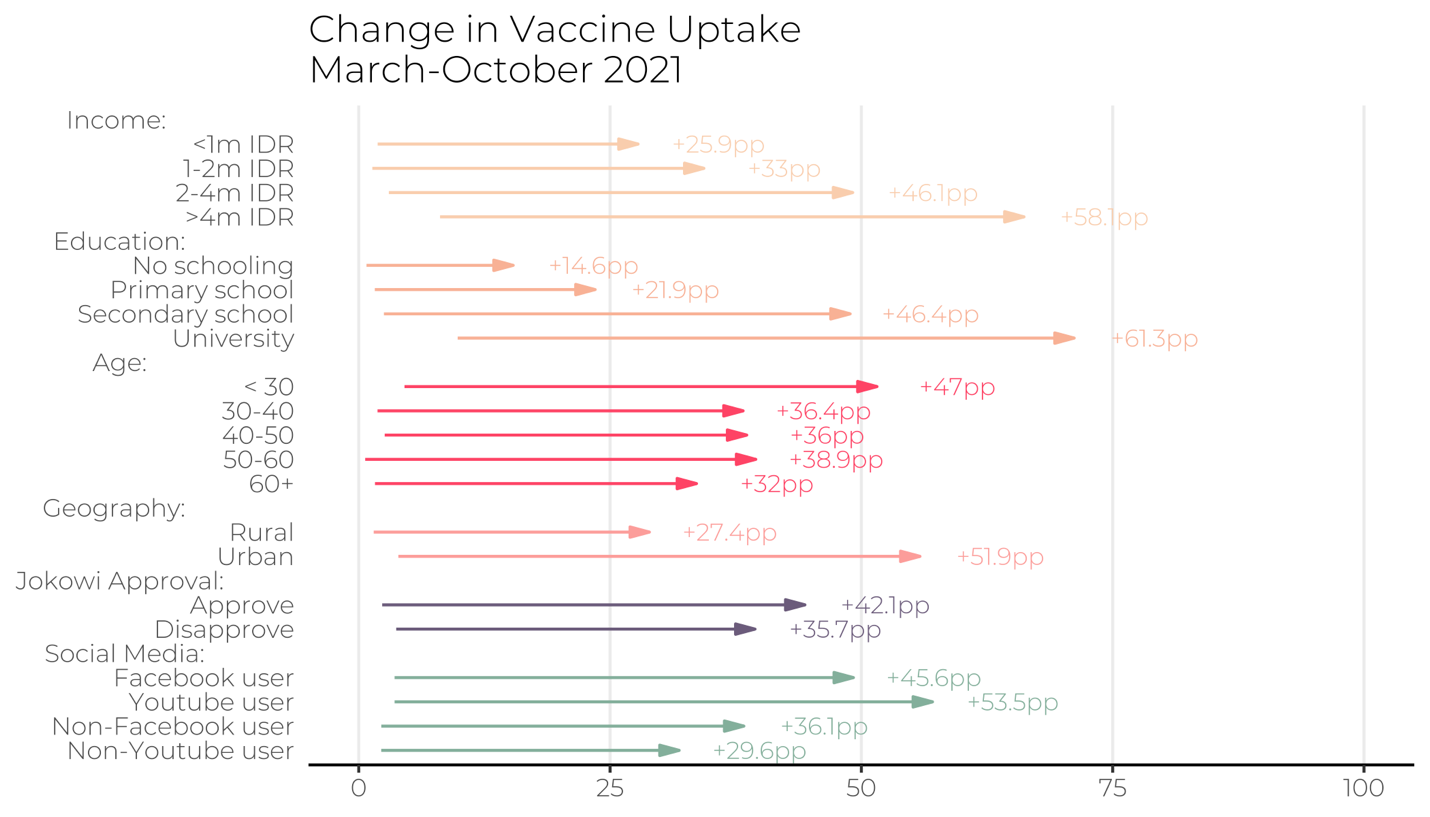
In surprising contrast with other countries—where vaccine rollouts targeted older citizens first—Indonesians under 30 are significantly more likely to be vaccinated (51.6%) than their older counterparts. Given that COVID-19 is more likely to result in severe illness or death for the elderly, it is particularly concerning that only 33.6% of Indonesians older than 60 had received a dose of the vaccine by the fielding of the survey.
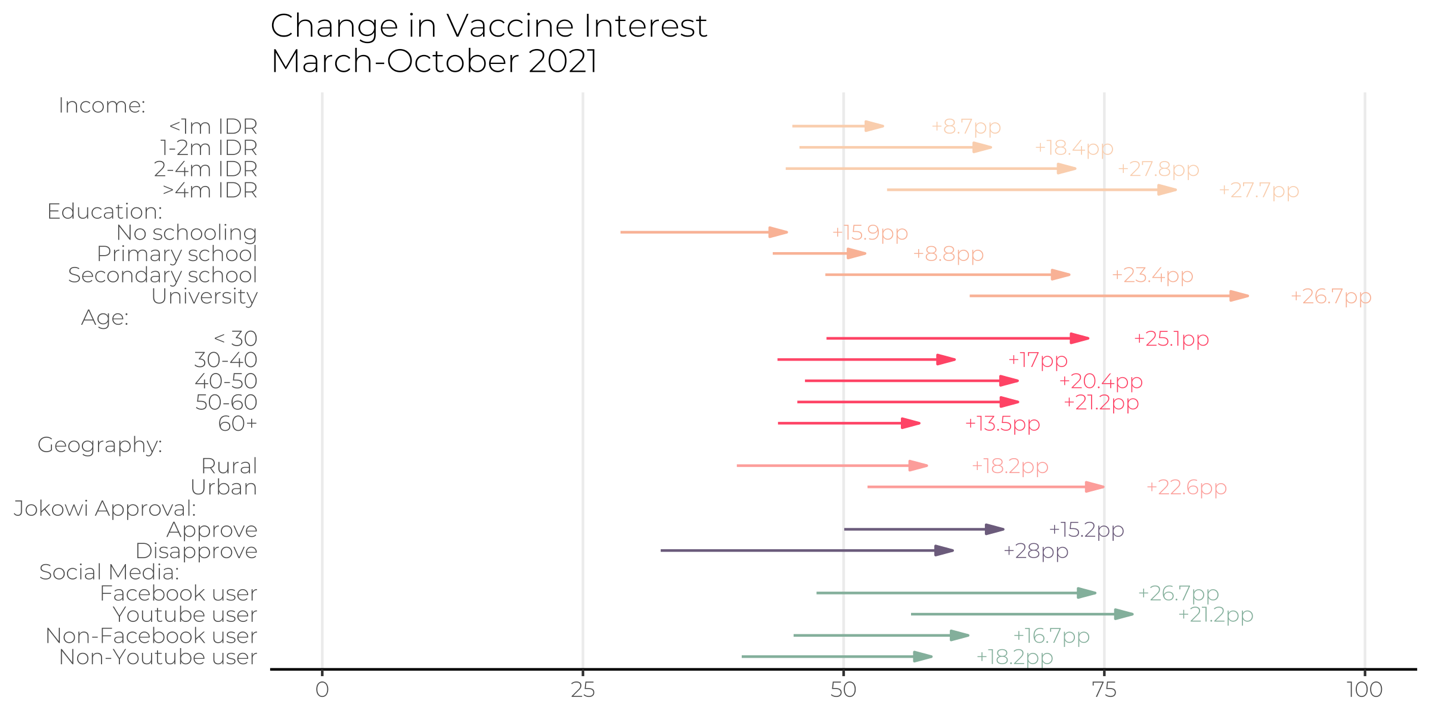
To get a better grip on whether these differential rates of vaccination reflect access or interest, in Figure 2, we also look at the share of respondents in each subgroup who expressed interest in getting a vaccine if offered. Here, we see the same trends observed in which respondents are getting vaccinated. A full 88.8% of university graduates, for instance, expressed an interest in getting vaccinated in October 2021 if it was made available—approximately twice as high as the percentage of respondents with no formal schooling (44.5%). Worryingly, the largest upticks in vaccination interest between March and October 2021 were among those who were, from the outset, more interest in getting vaccinated. Among individuals who make more than 4m IDR/month, interest in getting vaccinated increase by 51% over the seven months, compared to an 19.2% uptick in interest among individuals who make less than 1m IDR a month.
Why don’t some people want the vaccine in Indonesia?
What explains the lack of interest in getting vaccinated on the part of those respondents who indicated no intention of seeking out the jab? Recent accounts have placed considerable weight on the role of misinformation that has been circulating on social media. Looking at ten countries across the Global South, a team of researchers found widespread evidence of vaccine hesitancy motivated in part by false information held by respondents about the vaccines. Indonesia is no different: rumors have swirled on social media that the Chinese Sinovac vaccine is not halal, despite official statements to the contrary.
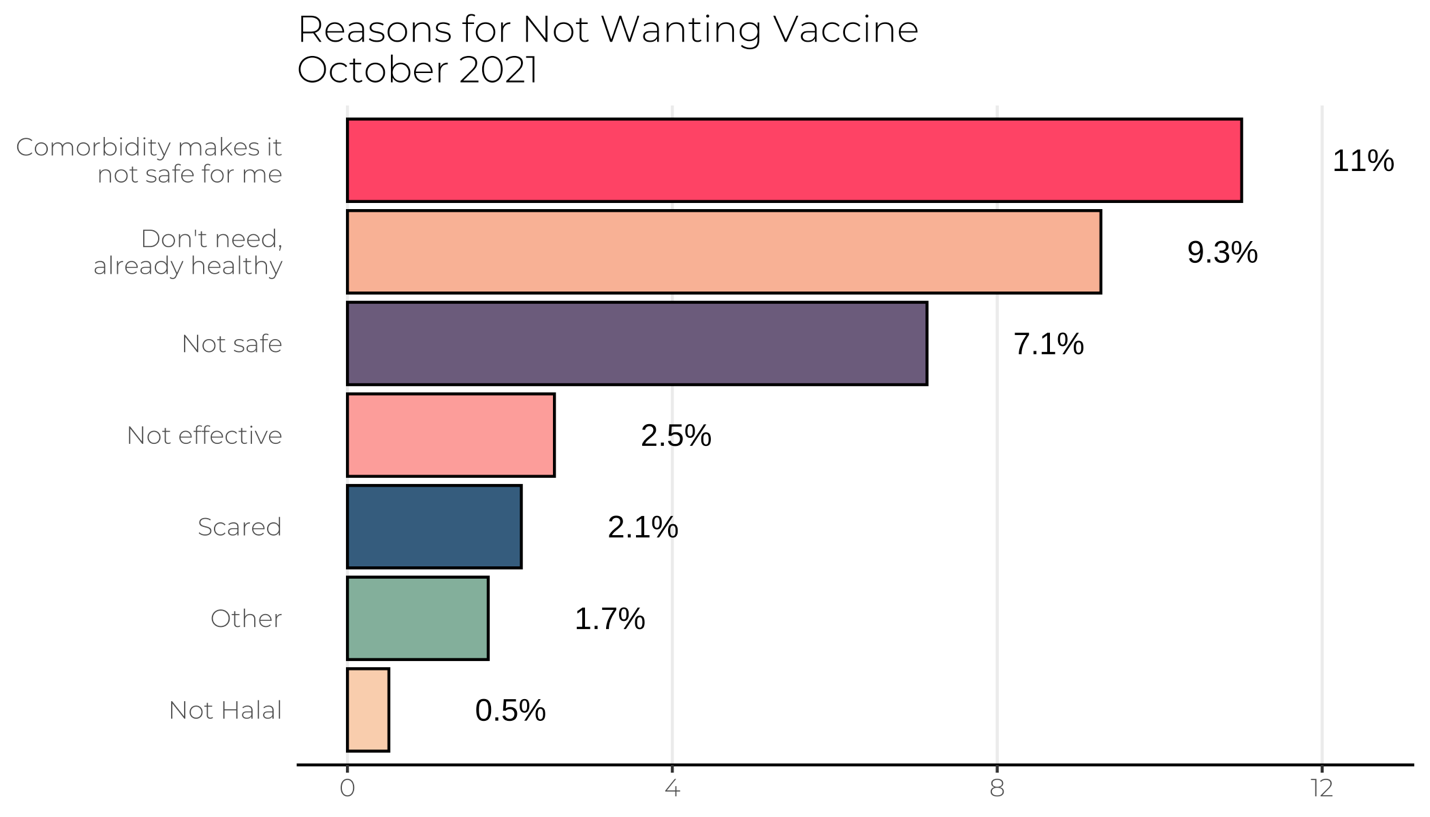
We therefore quizzed respondents who indicated no interest in getting vaccinated about their reason for opting against the jab. Respondents were able to choose from one of several reasons. In Figure 3, we show the percentage of the population indicating any one of the reasons listed. First, we find little evidence that a concern over vaccines not being halal is driving vaccine hesitancy: only 0.5% of respondents in our sample indicated this reason. Instead, the most common reason cited for not having an interest in getting vaccinated is respondents stating that their underlying comorbidity’s make vaccination unsafe—a concern likely motivated by concerns over side effects of the jab. In one sense, this is a line of misinformation that should be easily targeted with educational campaigns—as compared with more malevolent forms of misinformation regarding the providence and intention of vaccines.
Finally, we consider why it might be the case that older respondents indicate the lowest interest in vaccination in Indonesia. This is particularly puzzling: it is well documented that the older individuals are at greater risk of severe illness if infected with COVID-19. In theory, risk ought to be an important motivator to seek out vaccination. Indeed, it is precisely this tendency that has undermined the vaccine rollout in the United States, where many young people have opted to not get vaccinated, wagering that they are at lower risk to experience serious illness in the event they contract COVID-19.
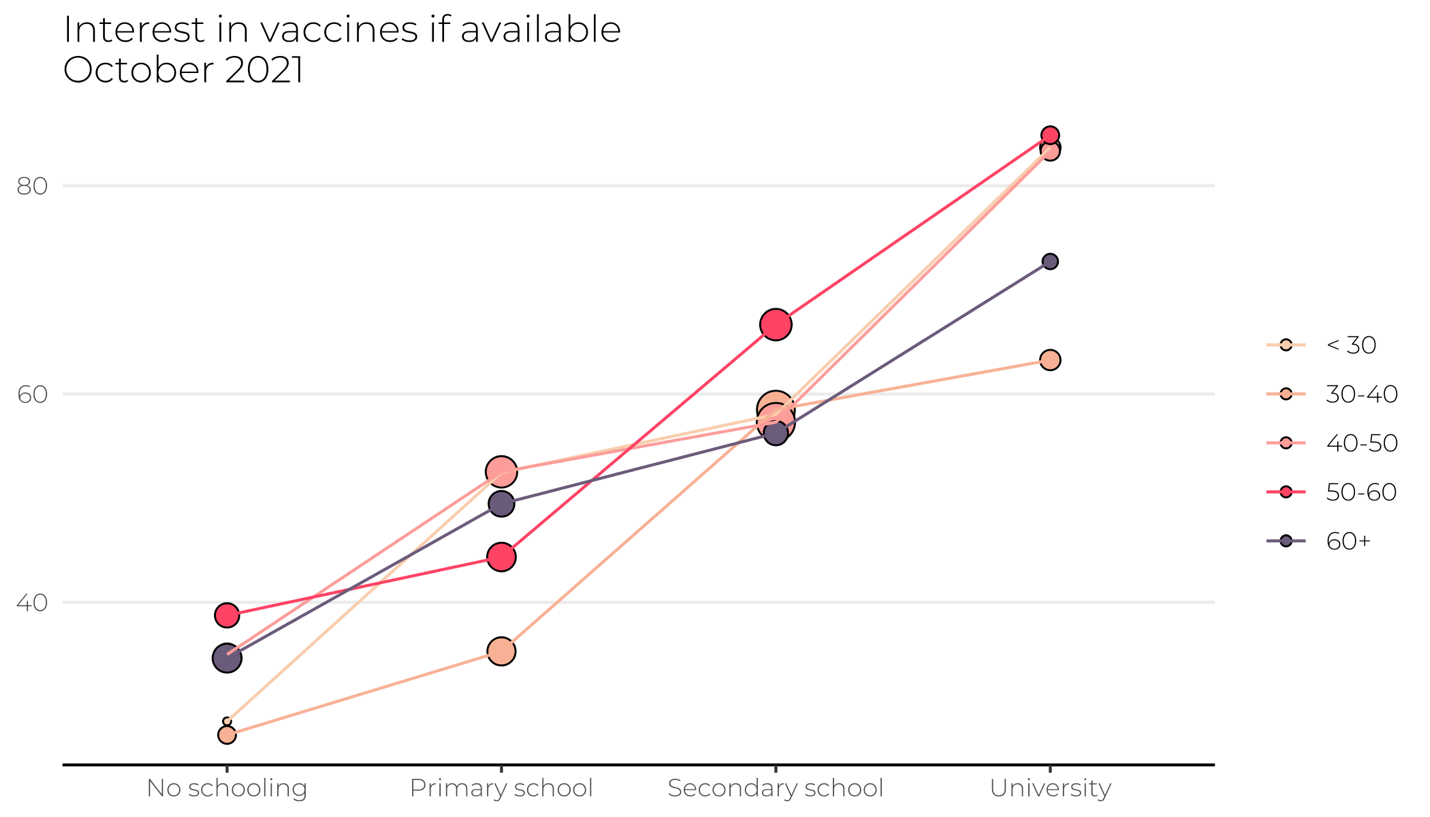
We examine the possibility that Indonesia’s geriatric bias in vaccination reflects the tendency for young people to be, on average, more educated than their seniors. It is well-documented that access to education has expanded over the past half century in Indonesia, and it may be that this expanded access has led to greater confidence and literacy in the recommendations of medical and scientific experts.
Indeed, consistent with this expectation, we find that education is the strongest predictor of interest in vaccination—above and beyond the role of age. Individuals who obtained at least a university degree—including those older than 60—are significantly more likely to express a desire to receive the jab than their less educated peers.
These findings provide important cues for policymakers looking to boost the overall rate of vaccination in Indonesia: for one, concerns over misinformation suggesting that vaccines are not halal appear to be overstated, and health authorities should instead focus their attention on remedying the notion that vaccine side effects are more dangerous than COVID-19 itself. Of course, this analysis is also subject to certain limitations. For one, the data are collected from a specific temporal point in the pandemic and vaccine rollout. Although we anticipate that many of the trends continue to hold, our research attests to the importance of conducting routine studies of the sources of vaccine inequity in Indonesia



