 Facebook
Facebook  Twitter
Twitter  Soundcloud
Soundcloud  Youtube
Youtube  Rss
Rss 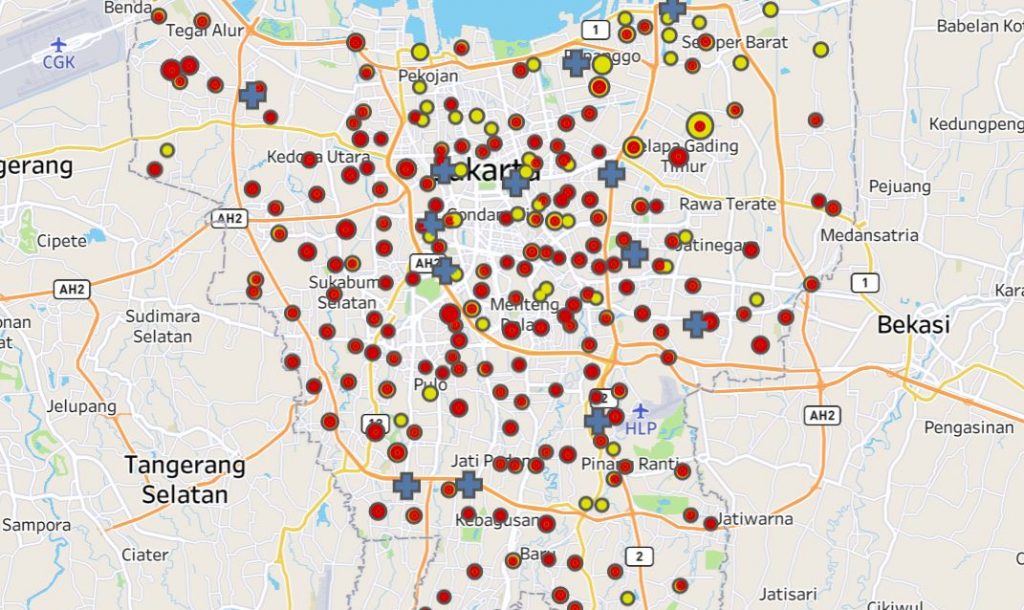
The policy and programmatic challenges presented by COVID-19 are testing Indonesia’s system of governance on multiple fronts.
The virus has inevitably exposed areas of weakness in the system, including administrative coordination between levels of government and the collection and management of data. However, the division of authority between the centre and the regions in relation to public health—and in particular, the power to authorise socially and economically disruptive measures to arrest the spread of communicable diseases—was arguably not predestined to be among those weaknesses.
This new report looks back at events in Indonesia during the first six months of 2020 to examine how Indonesia’s framework for centre-regional relations facilitated or hindered timely and coordinated action to mitigate the impacts of COVID-19. It finds that the current arrangements served to slow initial local responses to the pandemic without a corresponding payoff in the form of better national coordination.
But it did not have to be this way. A central government more intent on curbing the spread of the virus should have been able to work within that framework (or make subtle adjustments to it) to minimise delays in the application of public health measures. Instead, the central government displayed a curious knack for inserting itself into the process where greater regional discretion may have been appropriate, while absenting itself where a more active coordinating role would have been beneficial.
Click on the image to download the report.
Indonesia’s legal frameworks for COVID-19 response
The report begins by describing the two legal frameworks that have shaped Indonesia’s COVID-19 response: one general and pre-existing, the other specific and enacted in response to the pandemic. The former comprises an interlocking web of laws and regulations that define the scope of public health and emergency management measures available to policymakers and assign authority to impose those measures between different levels of government.
Decision-making authority under this framework is weighted heavily in favour of the central government, with regions largely responsible for implementation. Notably, the power to authorise measures such as the closure of schools or workplaces (components of what are known as large-scale social restrictions or PSBB) and more stringent restrictions on movement (generally understood as lockdowns) rests solely with the Minister of Health. Regional governments must seek approval from the Minister before applying these measures. Alternatively, the Minister can mandate their application by regional governments at his or her discretion.
A range of additional legal measures were also put in place to deal specifically with the unique public health, economic and social challenges posed by COVID-19. Of particular relevance to centre-regional relations was the establishment of a National COVID-19 Taskforce (subsequently subsumed within a National COVID-19 Committee) to coordinate Indonesia’s COVID-19 response both within and between levels of government. Regional governments were likewise required to establish their own COVID-19 taskforces, headed directly by the governor, district head or mayor. A range of other laws, regulations, decrees and instructions have also been issued to address particular regulatory needs.
What did Indonesia gain and lose from a centralised decision-making approach?
Regional government capacity varies significantly across the Indonesian archipelago. And with communicable diseases such as COVID-19 unconstrained by administrative boundaries, there are good arguments in favour of the central government retaining ultimate authority over the imposition of public health measures such as PSBB and lockdowns. Idiosyncratic or reckless decision-making by any of Indonesia’s 514 districts and municipalities could have serious national consequences for both public health and the economy.
But what if the opposite occurs, and it is the central government dragging its feet? As is now well known, this was the situation facing Jakarta’s more proactive governor Anies Baswedan in March when the virus was first detected in Indonesia. The report draws primarily upon this example to illustrate sites of tension and decision-making bottlenecks arising from the way in which authority to impose significant public health measures is divided between levels of government. Two key points emerge.
First, the requirement for regions to seek Ministerial approval to apply PSBB—including the convoluted administrative process for doing so—led to largely avoidable delays when time was of the essence. In the case of Jakarta, two weeks were lost between Baswedan’s initial request for a lockdown and the commencement of PSBB. Greater regional discretion over the application of public health measures could facilitate quicker responses and provide partial insurance against central government inaction (a central government intent on vetoing regional action would retain the power to do so). The central government would also retain the power to direct regions to take action if necessary.
Second, while centralised decision-making may tend to privilege coordination over speed, in the early stages of the pandemic the central government sacrificed the latter without a discernible improvement in the former. Jakarta again provides an obvious example. Despite administrative boundaries being irrelevant to the spread of the virus, the central government declined to use its authority to apply PSBB over the greater Jakarta area (which includes satellite cities in the neighbouring provinces of West Java and Banten). Instead, it largely left governors, mayors and district heads to sort it out amongst themselves.
The extent to which any of this has significantly altered the trajectory of COVID-19 in Indonesia is a different question. Considering events since, the ultimate impact may not have been that great. Leadership (or lack thereof) has arguably been more influential. But it remains useful to reflect on how the division of authority between the centre and the regions might be refined in order to provide governments at all levels the best opportunity of mounting timely and effective public health responses throughout the remainder of this pandemic and/or when the next one inevitably strikes.
Viewed more broadly, the Indonesian case also adds weight to more general observations about the influence of systems of governance on national responses to COVID-19. Whether unitary or federal, centralised or decentralised, system design entails trade-offs. These have consequences—both positive and negative—but are not necessarily determinative of a particular outcome. Many other factors are also at play. In Indonesia’s case, a significant factor has been how policymakers have decided to use (or not) the policy levers at their disposal. And that is something that the no system—however well designed—can do on their behalf.



